
Approach to Management of PPH following Cesarean Section
I. Cesarean Section Delivery with 1000-1500mL estimated blood loss, with ongoing excessive bleeding and/or mild tachycardia and/or hypotension.
Consider 4 T’s:
- Tone: GA may cause uterine atony ,prolonged labour, chorioamnionitis, polyhydramnios
- Tissue: rule out abnormal placentation
- Trauma: Manual and visual exploration of cavity to check for bleeding site, uterine incision extension, uterine artery laceration etc
- Thrombin: patient history
Approach:
- Notify the team (anesthesia, lab, nurses, consider calling referral centre/transport)
- Determine likely etiology (tone, tissue, trauma, thrombin)
- Bimanual compression and uterotonics (oxytocin, carboprost, ergometrine, misoprostol, txa, vasopressin)
- Crossmatch, activate MTP(massive hemorrhage protocol), fluids
- Consider Bakri and uterine packing
- Resort to B-Lynch suture and other compression sutures earlier rather than later

- Check for “concealed” blood loss per vaginum
- Uterine artery ligation
Equipment list
- Kerlix gauze, packing forceps
- Goodwin bundle (ring forceps, right angle retractors for the lateral vaginal walls, weighted speculum, chest needle drivers, long scissors)
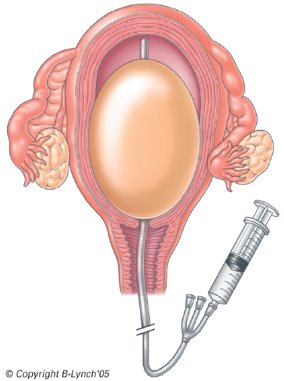
- Intracavitary (Bakri) balloon
- Suture for B Lynch (eg. #2 Vicryl on a 70mm curved needle)
PEARL: PACKING TECHNIQUE
Consider uterine packing with layers of Kerlix gauze tucked into the cornua and systematically layered down to the lower uterine segment. If more than one gauze length is required, a secure square knot is made between the two ends and layering is continued. The end of the gauze it passed through the cervix into the vagina before the uterine incision is closed. Be aware of infection risk, potential of ongoing unrecognized bleeding and potential repeated surgery for packing removal
PEARL: LOWER SEGMENT UTERINE BLEEDING:
- Uterotonics do not help as lower segment is non-contractile
- Bakri (single) balloon may not be enough so vagina needs tamponade in order to compress the lower segment
Strategies:
- Use a device with vaginal balloon,
- Pack the vagina tightly with layers of Kerlex gauze and insert a Foley into the urethra
- Try inflating a blood pressure cuff in a bag in the vagina
PEARL: TEMPORIZING MEASURES
Uterine tourniquet,
manual aortic compression
clamps across utero-ovarian ligaments
II. Cesarean Delivery with >1500mL blood loss, with ongoing excessive bleeding and/or hemodynamic instability.
If previous interventions unsuccessful be ready for peripartum hysterectomy
Emergency postpartum hysterectomy section